
I'm Isaac Saul, and this is Tangle: an independent, nonpartisan, subscriber-supported politics newsletter that summarizes the best arguments from across the political spectrum on the news of the day — then “my take.”
Are you new here? Get free emails to your inbox daily. Would you rather listen? You can find our podcast here.
Today’s read: 14 minutes.
Browse Like It's Y2K
Remember when "pop-ups" meant toys, not annoying ads?
Back when the only thing tracking you was your neighbor's nosy cat?
Today's internet is loud, cluttered, and secretly collecting your data. CleanWeb from Surfshark is the digital bouncer you never knew you needed.
It blocks ads, trackers, and malware. Just one install, and boom — pages load faster, creepy banners disappear, and your browsing feels like the internet used to: clean, simple, and yours.
Tangle readers can get it now for just $1.99/month (87% off), plus enjoy 3 extra months free.
*This is a sponsored post.
Want to get texts from Tangle?
Since October, over 13,000 Tangle readers have joined us on Subtext, our free SMS messaging service that lets us connect directly with readers. Subtext subscribers can weigh in on our coverage through topic polls, receive analysis on developing stories straight from Isaac, and get occasional peeks behind the scenes at Tangle’s operations. You can sign up for Subtext here!
(Note: Subtext is currently only available for subscribers based in the U.S. and Canada.)
Quick hits.
- Congress released a bipartisan government funding bill ahead of the January 30 deadline to avoid a shutdown. Democrats in the House and Senate are expected to challenge provisions for the Department of Homeland Security, seeking further reforms to Immigration and Customs Enforcement’s operations. (The bill)
- At the World Economic Forum on Wednesday, President Donald Trump pledged not to use military force to take Greenland but continued to insist that controlling the island is critical for U.S. security. (The speech) On Tuesday, Canadian Prime Minister Mark Carney addressed the gathering, alluding to the Trump administration’s actions as causing a “rupture” in the world order. (The address)
- The Justice Department subpoenaed six Minnesota government offices — including the Governor’s Office, the Attorney General’s Office, and the Minneapolis Mayor’s Office — amid its investigation into alleged efforts to obstruct federal immigration operations in the state. (The subpoenas)
- Attorney General Pam Bondi announced that Lindsey Halligan is leaving her role as interim United States attorney for the Eastern District of Virginia. Halligan had brought charges against former Federal Bureau of Investigation Director James Comey and New York Attorney General Letitia James (D), but courts dismissed the cases after finding Halligan was illegally appointed. (The departure)
- Australia’s parliament passed a series of gun control laws in response to the mass shooting that killed 15 people at a Hanukkah celebration at Bondi Beach in Sydney in December. The new laws create a national gun buyback program, limit imports of firearms, and enhance background checks. (The laws)
Today’s topic.
Trump’s healthcare plan. On Thursday, January 15, President Donald Trump announced several proposals to lower health insurance costs, which he called “The Great Healthcare Plan.” The healthcare-reform framework focuses on four broad initiatives: lowering drug prices, lowering insurance premiums, holding big insurance companies accountable, and maximizing price transparency. Although the White House has not announced specific legislative proposals to enact the policy, Trump specified he would seek to make more medications available over the counter, regulate pharmacy benefit managers (PBMs), and require insurance companies to explain their costs in simple and clear language.
Separately, on Tuesday, Congressional leaders reached a bipartisan deal in both chambers to advance a four-bill “minibus” spending package that includes several healthcare stipulations. The spending bills set funding levels for the Departments of Defense, Transportation, Labor, Health and Human Services (HHS), and Homeland Security; the HHS bill limits PBM benefits, extends telehealth coverage, and extends funding for at-home Medicare and Medicaid services through 2030.
Back up: The healthcare deal revives a 2024 bill — scuttled by then-President-elect Trump and Elon Musk over spending concerns. The new spending bill pursues many of the same goals as its predecessor; it also does not take up the Affordable Care Act (ACA) subsidies, which expired at the end of 2025 and were central to last year’s prolonged government shutdown. Democrats proposed extending the expanded benefits for three years in a bill that passed the House on January 8 but has since stalled in the Senate.
We previously covered the government shutdown here and the expiring ACA benefits here.
The path to enacting the proposals in the president’s Great Healthcare Plan is unclear, and statements from Republicans indicate that changing the current bipartisan spending agreement would be difficult. “You’re going to need 218 votes, which means you’re going to need to build consensus across the conference on what it is we’re pursuing,” Rep. Mike Lawler (R-NY) said. Sen. Josh Hawley (R-MO) called the GOP’s healthcare options “pretty limited.”
Democrats dismiss Trump’s framework as ineffective. “Trump’s ‘Great Healthcare Plan’ does nothing to substantively bring down health care costs,” Democratic National Committee Rapid Response Director Kendall Witmer said.
Below, we’ll get into what the left and right are saying about the president’s healthcare plan and Congress’s spending bill. Then, Senior Editor Will Kaback gives his take.
What the left is saying.
- Many on the left are critical of the healthcare plan, arguing that it has little substance.
- Some argue that the plan doesn’t lay out a clear legislative strategy.
- Others say that Trump’s proposals won’t lower healthcare costs.
In Public Notice, Paul Waldman said “Trump’s long-awaited healthcare ‘plan’ is a joke.”
“[The plan] does contain a few things that look like big ideas, but are immediately baffling,” Waldman wrote. “The biggest is this one: ‘The government is going to pay the money directly to you,’ the plan quotes Trump saying. ‘It goes to you, and then you take the money and buy your own healthcare.’ How exactly is that going to work? We’ll each get a check every month from the government? Is the entire insurance system going to be replaced by health savings accounts? Worry not: Trump insists that prices will come down, because he says you’ll ‘go out and buy your own healthcare, and you’ll make a great deal.’”
“It’s quite clear that if someone asked Trump to name two things his ‘plan’ does, he would not be able to. This has been one of the defining features of healthcare policymaking in both Trump terms: He not only knows almost nothing about the issue, he has no evident beliefs about healthcare; in fact, he couldn’t care less about it,” Waldman said. “Trump does, however, have a simplistic but basically accurate understanding of what the public wants, so when speaking off the cuff he’ll say things that make him sound almost liberal. But when it comes time to produce something that vaguely resembles a policy blueprint, Trump steps aside and the right-wing ideologues who surround him take over.”
In The Bulwark, Jonathan Cohn wrote that “Trump’s ‘Great Healthcare Plan’ is not great. It’s not even a plan.”
“Trump’s poll numbers are in the dumps, with voters identifying the high cost of living as a top concern. That includes the price of health care, which just went up for more than 20 million Americans who rely on the Affordable Care Act,” Cohn said. “Negotiations [over enhanced ACA subsidies] have since stalled, making Thursday’s plan the latest in a series of chances for Trump to weigh in strongly on what he wants. And at first blush it looked like Trump might do just that, finally, because he endorsed two key ideas that Republicans have been discussing in the debate over extending the subsidies.”
“One — which has gotten a fair amount of attention — would take at least some of the money from those extra subsidies and put them instead in tax-favored spending accounts that people can use on health care. The other idea Trump endorsed is a call to provide funding for something called ‘cost-sharing reductions,’” Cohn added. “The endorsement of these ideas was conspicuously half-hearted. It’s possible Trump and his advisers were making a conscious, strategic choice not to slam the door on anything that might come out of the bipartisan talks on Capitol Hill. But staying out of the process isn’t going to get a deal done, either, because getting to sixty votes in the Senate would almost certainly require pressure on Republicans hesitant to support any extension of the subsidies.”
In Common Dreams, Eagan Kemp argued the plan “is doomed to fail — we need Medicare for All.”
“President Donald Trump’s new ‘Great Health Care Plan’ is anything but,” Kemp wrote. “Unsurprisingly, Trump’s concepts of a plan fail to even begin to reverse the damage he caused when he made massive cuts to Medicaid and the Affordable Care Act in order to fund tax cuts for billionaires. Now, Trump and his Republican allies are trying to cover up the gaping wound they have created with a Band-Aid. At the same time, Americans are desperate for relief from Trumpflation, including rapidly rising healthcare costs.”
“Shutdown negotiations and subsequent scattershot health ideas from the White House and Republicans in Congress show they have no real idea what to do when it comes to actually bringing down the cost of healthcare in America… The only alternate Republican plans for healthcare that currently exist strictly serve corporations and fail to provide relief to patients,” Kemp said. “Fortunately, Medicare for All would address all of these issues and finally put the health of Americans ahead of corporate profits. Medicare for All would guarantee that everyone in the US can get the care they need when they need it, without financial barriers or hoops to jump through, and would be cheaper than our current system while providing coverage that is better than any commercial health insurance plan.”
What the right is saying.
- The right sees Trump’s healthcare plan as a mixed bag.
- Some say the document falls short of an alternative vision to Obamacare.
- Others endorse direct payments to Americans over ACA subsidies.
In The Federalist, Christopher Jacobs described “the good, the bad, and the ugly of the White House health plan.”
“In theory, sending money to patients rather than insurance companies will give the American people greater control over their health care choices, while promoting competition,” Jacobs wrote. “Likewise, proposals to allow more pharmaceuticals to be sold over-the-counter hold some appeal. Expanding the [over-the-counter] marketplace could increase competition, while also lowering health care costs by eliminating additional trips to the doctor to obtain prescriptions. By contrast, Obamacare included language (since repealed) requiring people to obtain a prescription to have OTC medicines reimbursed from a Flexible Spending Arrangement or Health Savings Account, which resulted in a rush of unnecessary appointments where patients asked for ‘prescriptions’ for things like NyQuil.”
“Proposals to increase transparency — requiring insurers to explain their plans in plain English, publish their rates of treatment denials, and publicize their percentage of administrative overhead, and mandating providers to publish their prices — should help at the margins. The proposal to fund the cost-sharing reduction program falls into a similarly ambivalent category,” Jacobs said. “The worst of the White House proposals concerns policies to codify the president’s Most Favored Nation deals… American patients deserve lower health care costs, which several policies in the president’s health care plan would achieve. They don’t deserve arbitrary discrimination against the most vulnerable, which could result from codifying the White House’s price control plan.”
The National Review editors wrote about “Trump’s not so great health-care plan.”
“President Trump deserves credit for thus far resisting Democrats’ demands to throw more money at the failed Obamacare program. But on Tuesday, he offered a one-page policy response, characteristically titled, ‘The Great American Healthcare Plan,’ that leaves much to be desired,” the editors said. “The outline is mostly small-bore ideas that range from inadvisable (importing socialist price controls for pharmaceuticals) to perfectly fine but inadequate (allowing more drugs to be purchased over the counter and expanding price transparency). The plan misses because ultimately it doesn’t offer a contrary vision for health care from Obamacare.”
“It would be great if Americans had more control over health-care dollars and had the ability to choose from more plans. But absent broader changes on the regulatory front, enrollees wouldn’t have a real choice as they would still be purchasing among Obamacare plans,” they added. “To be clear, if the Trump health-care outline serves the purpose of steering antsy Republicans away from a catastrophic decision to join Democrats in expanding Obamacare, that alone would be a net positive. But as an alternative vision for health care, it isn’t big, beautiful — or great.”
In Reason, J.D. Tuccille said the plan “has promise but should add more freedom for Americans.”
“‘The Great Healthcare Plan’ doesn’t really undo the bad government interventions and restrictions that limit choice and raise costs. The plan might offer some improvement over what we have, but it should be a lot better. In fact, legislation that would greatly improve the plan has already been presented to Congress,” Tuccille said. “Critics of what we’ve seen of the Great Healthcare Plan worry that it just builds a little more transparency and a few more options — plus added subsidies — into existing Obamacare distortions of the medical marketplace.”
“A good place to start in terms of fleshing out the health care plan with details that would expand choice and patient freedom and lower costs is Sen. Rand Paul’s (R–Ky.) ‘Health Marketplace and Savings Accounts for All Act,’ introduced last month,” Tuccille wrote. “The bill raises the annual contribution cap on tax-advantaged Health Savings Accounts (HSAs) from $4,400 for individuals and $8,750 for families to $24,500 and extends HSA eligibility to everybody. It also expands what HSAs can cover. Basically, Paul’s bill would dramatically increase Americans’ control over their health care money and make their coverage portable by delinking it from employment.”
My take.
Reminder: “My take” is a section where we give ourselves space to share a personal opinion. If you have feedback, criticism or compliments, don't unsubscribe. Write in by replying to this email, or leave a comment.
- Trump still doesn’t have a healthcare plan that we can evaluate in depth.
- Congress is already considering similar ideas, but it’s not clear where Trump’s plan fits in.
- I’m left disheartened about the prospects for serious healthcare reform.
Senior Editor Will Kaback: President Trump’s healthcare plan fell out of the headlines as quickly as it appeared. That’s understandable — Greenland, anti-ICE protests, and the second phase of the Gaza ceasefire plan are just a few of the major stories that have supplanted it — but the relatively quiet response from lawmakers and commentators to the plan is still surprising. After all, one of the most memorable moments of the 2024 presidential campaign was Trump saying he had “concepts of a plan” for healthcare, an assurance that has remained about that vague for roughly a decade. Now Trump has finally introduced his proposal, and the reaction seems almost muted. What gives?
First off, “The Great Healthcare Plan” (GHP) is a misnomer — it’s a loose framework, the kind of document that works well as a page on a campaign website but not as a baseline for actual legislative reform. While it puts forward some big ideas, Trump’s proposal is short on details and shorter on a policy approach. Several of its prescribed reforms are intriguing, but the dearth of fleshed-out policies makes it difficult to evaluate — a reaction that commentators on both sides shared above.
After diving into the responses to Trump’s announcement, a few things are clear: The GHP is not the Affordable Care Act “replacement” Trump has long promised, it’s unlikely to be adopted wholesale by Republican lawmakers, and it fails to address many core issues in our healthcare system. It is more of a gesture toward popular reforms without any action, an agreeable wishlist without a commitment to the tradeoffs or political strategy required to enact anything substantial.
Though the GHP is not a cohesive reform agenda, some of its ideas overlap with real legislative efforts worth examining. Most notably, Trump is pushing to codify his deals on prescription-drug prices, some Senate Republicans are mobilizing on the call to replace ACA subsidies with direct individual payments, and Congress’s recent bipartisan healthcare funding agreement includes a crackdown on pharmacy benefit managers (PBMs).
I have mixed thoughts on each of these proposals. Let's take them one by one.
On drug prices, the GHP leads with a push for “Most-Favored-Nation” (MFN) deals — compelling pharmaceutical companies to sell their products at the lowest price that they are sold for in other countries. Trump signed an executive order last May directing the Department of Health and Human Services to facilitate these price targets for pharmaceutical companies, and at the end of 2025, he announced voluntary pricing agreements with nine major manufacturers to bring down drug prices. However, those same companies recently announced price increases for 872 different name-brand medications. The White House says that the negotiated price reductions are coming to state Medicaid programs and patients who pay in cash for some prescriptions, but the episode underscores how only legislation, not executive action, can address drug prices.
Relatedly, codifying MFN requirements isn’t guaranteed to bring down prices either — whether through executive order or new legislation. Americans really do pay much higher drug prices than citizens of other countries, and this policy does have strong support from the left. But the plan relies on a few risky assumptions — that drug companies wouldn’t pull drugs from the market rather than lower prices or raise prices abroad rather than lowering them in the U.S. I’m less concerned about the risk of stifling innovation (a core concern on the Republican side), as recent studies estimate that similar proposals would have a small impact on the number of new drugs coming to market in the long run. In sum, codifying MFN pricing sounds good in the abstract, but Trump’s plan offers no details to account for these potential pitfalls in practice.
On the GHP’s direct payments to individuals, these are effectively a replacement for the enhanced ACA subsidies that expired at the end of 2025 (and that Democrats are fighting to reinstate). Sen. Bill Cassidy (R-LA) has offered the most detailed proposal for turning this idea into legislation, rerouting the funds for the subsidies to individual health-savings accounts (HSAs) that cover out-of-pocket healthcare costs. However, as some Democrats and health-policy experts have noted, these savings accounts are only available through plans that carry higher co-pays and deductibles than others. In effect, this would reduce the savings provided by covering out-of-pocket costs by forcing people onto the plans with the highest co-pays and deductibles — all without addressing the persistent problem of rising premiums. Perhaps these issues could be addressed with additional reforms, but we haven’t seen them; Cassidy’s plan hasn’t been written up as a bill, and the GHP offers no more guidance.
Lastly, PBMs. The bipartisan healthcare package legislators reached on Tuesday includes, among other measures, an overhaul of PBM practices. Today, PBMs decide which drugs are covered by insurance, meaning that they can earn more when they approve coverage for more expensive drugs, because drug companies often give bigger discounts on higher-priced medications (and PBMs keep part of that money). The new provisions would instead require PBMs to be paid a flat fee for their services and to pass along any discounts they get directly to health insurers (instead of keeping those discounts for themselves). Of all the ideas raised by the GHP with some legislative momentum, PBM reform seems like the best place to start, removing warped incentives that lead to increased costs across the healthcare system.
But does the GHP actually help with this effort? Without a clear legislative strategy from the White House, it’s unclear whether Trump wants to save PBM reform for a comprehensive, to-be-realized healthcare bill or whether he’s content with Congress passing different elements of the proposal in piecemeal fashion. Knowing the president, he probably prefers the former, which makes it surprising that the rollout of this plan has been so lackluster. I can only speculate, but my impression is that the administration lacks the political will for a bruising healthcare fight with so much of its attention focused abroad, and this half-hearted plan signals to Congress that it should take up the reins. That could still change, but with the midterms fast approaching, Trump’s promise of comprehensive healthcare reform seems less and less likely to ever materialize.
Another thought stuck in my mind as I was reading commentary from writers on the right and left: All of the analysis I read — from experts and editorial boards and legislators considering their options — took healthcare reforms more seriously than Trump’s proposal itself. And that’s deeply disheartening. Just over a year ago, UnitedHealthcare CEO Brian Thompson’s killing laid bare millions of Americans’ deep-rooted frustrations with our healthcare system, and just a few months ago we had the longest government shutdown in U.S. history (purportedly on account of needed healthcare reforms). Despite lots of talk about action, we still seem to be dancing around the actual decisions of which reforms to prioritize and how to make them law.
Congress at least seems committed to some measure of reform, but where is the White House? Frankly, it’s shocking that a president who has been so willing to flex executive power and impose his will on lawmakers has chosen to punt so visibly on such a key issue. After years of promises, Americans were told the plan we have now would finally clarify the president’s vision for healthcare reform. Instead, it underscores how far we still are from a serious, sustained effort to fix a system nearly everyone agrees is broken.
Take the survey: Which healthcare reforms would you support? Let us know.
Disagree? That's okay. Our opinion is just one of many. Write in and let us know why, and we'll consider publishing your feedback.
Your questions, answered.
Q: I’ve seen several reports of DHS displaying supposed Nazi and KKK slogans: “One of ours, all of yours” and “We’ll have our home again.” What do you make of this?
— Jake from Grand Rapids, MI
Ari Weitzman, Managing Editor: I wanted to take this question as the member of Tangle’s staff who most vocally claimed, last year, that Elon Musk did not make a Nazi salute at Trump’s inauguration celebration. I still think it’s reasonable to disagree over that instance, but a month later, Steve Bannon unambiguously made a ‘sieg heil’ at CPAC, seemingly as a troll, and I said that “this mainstreaming of Nazi salutes, even sarcastically, is an enormous problem for the right.”
To risk egregious understatement, I’d say that problem has gotten worse.
Over the past 10 days, official social media accounts for the United States government have posted messages with clear parallels to Nazi propaganda. On January 10, the Department of Labor posted a short video on X with the caption, “One Homeland. One People. One Heritage,” an apparent reference to the Nazi slogan, “One People, One Empire, One Leader.” On January 13, Department of Homeland Security (DHS) Secretary Kristi Noem stood behind a lectern with the caption “One of ours, all of yours,” a slogan allegedly connected to the 1942 annihilation of Lidice in the Nazi Protectorate of Bohemia and Moravia. On January 14, the White House posted a cartoon on X asking, “Which way, Greenland Man,” referencing a book from 1978 that explicitly argued the inferiority of Africans and Jews.
All of these apparent references, on their own, are explainable. Three short statements beginning with the word “one” are not uncommon. The slogan DHS used was actually never used by Nazis and only loosely connected to the Lidice massacre. And “Which Way, Western Man” had already become a flexible meme format long before the White House’s tweet.
Then, on January 16, the Department of Labor posted on X, “We’ll never stop fighting for the American Way of Life. AMERICA FIRST. AMERICANS FIRST.” The first line uses German noun capitalization and is 14 words long (an apparent reference to two prominent neo-Nazi slogans known as the fourteen words); the whole post contains spacing that makes it 88 characters in total (another apparent neo-Nazi reference).
It strains credulity to dismiss this pattern — outside the Labor tweet and within it — as a string of innocuous coincidences. These are clearly Nazi dog whistles — signals intended for normal people to miss but Nazi sympathizers to hear. But why? Maybe employees who manage these accounts have coordinated these messages amongst themselves as edgy, in-group signaling. Maybe their supervisors don’t care — or, maybe, they intend the strategy to both wink at this poisonous portion of their base while castigating the rest of us who pick up on these subtle (yet troublingly consistent) patterns as hyperventilating pearl-clutchters.
In my opinion, that’s exactly what’s happening. When I asked DHS for comment on these examples, Assistant Secretary Tricia McLaughlin said, “Revolting. I already addressed this on CNN and you’re actually conspiracy theorists for giving this credibility.”
Want to have a question answered in the newsletter? You can reply to this email (it goes straight to our inbox) or fill out this form.
Under the radar.
China is the world’s second most-populous nation, but in 2025, its population shrank for the fourth consecutive year. According to government statistics released on Monday, China’s total population decreased by three million people, and the birth rate was 5.63 per 1,000 people, the lowest on record since 1949 and a 17% decrease from the previous year. People in China cite rising costs as a deterrent to having children, while experts have also pointed to the lingering effects of the government’s multi-decade “one child policy” that remained in effect until 2015. Though China is viewed as an ascendant world power, economists say its population challenges could hamper its long-term growth. The Associated Press has the story.
The Internet Used to Be Quieter
Remember browsing without pop-ups stalking you across every site? CleanWeb from Surfshark brings that back — blocking ads, trackers, and malware with one install.
Pages load faster, creepy banners vanish, and your data stays yours.
Tangle readers get it for $1.99/month (87% off) plus 3 extra months free.
Numbers.
- 16. The number of drug companies with whom Trump has struck “most-favored-nation” pricing deals in his second term, according to drug research firm 46brooklyn.
- $50 billion. The approximate amount President Trump’s Great Healthcare Plan would save the federal government over the next decade, according to estimates by the Committee for a Responsible Federal Budget.
- $36 billion. The amount of those savings that would come from funding cost-sharing reduction subsidies.
- $350 billion. The plan’s estimated 10-year cost to the federal government if it funds “extra taxpayer-funded subsidy payments” with money that would otherwise have gone to extending enhanced Affordable Care Act (ACA) subsidies.
- 1.4 million. The drop in ACA plan enrollment from January 2025 to January 2026, according to a Centers for Medicare and Medicaid Services report.
- 37% and 60%. The percentage of registered voters who approve and disapprove, respectively, of President Trump’s performance on healthcare, according to a January 2026 Wall Street Journal poll.
The extras.
- One year ago today we covered Trump’s inauguration.
- The most clicked link in yesterday’s newsletter was each state’s preferred breakup food.
- Nothing to do with politics: Some dogs can learn more words by eavesdropping on human conversations.
- Yesterday’s survey: 5,398 readers responded to our survey on Greenland with 31% saying it should remain a Danish region with ties to the U.S similar to the ones that currently exist. “We already have an agreement with the Danish government that allows us to have military bases and other uses,” one respondent said. “Seward was nuts for pursuing Alaska. Isn’t Greenland another valuable piece of land that’s been ignored for too long,” said another.
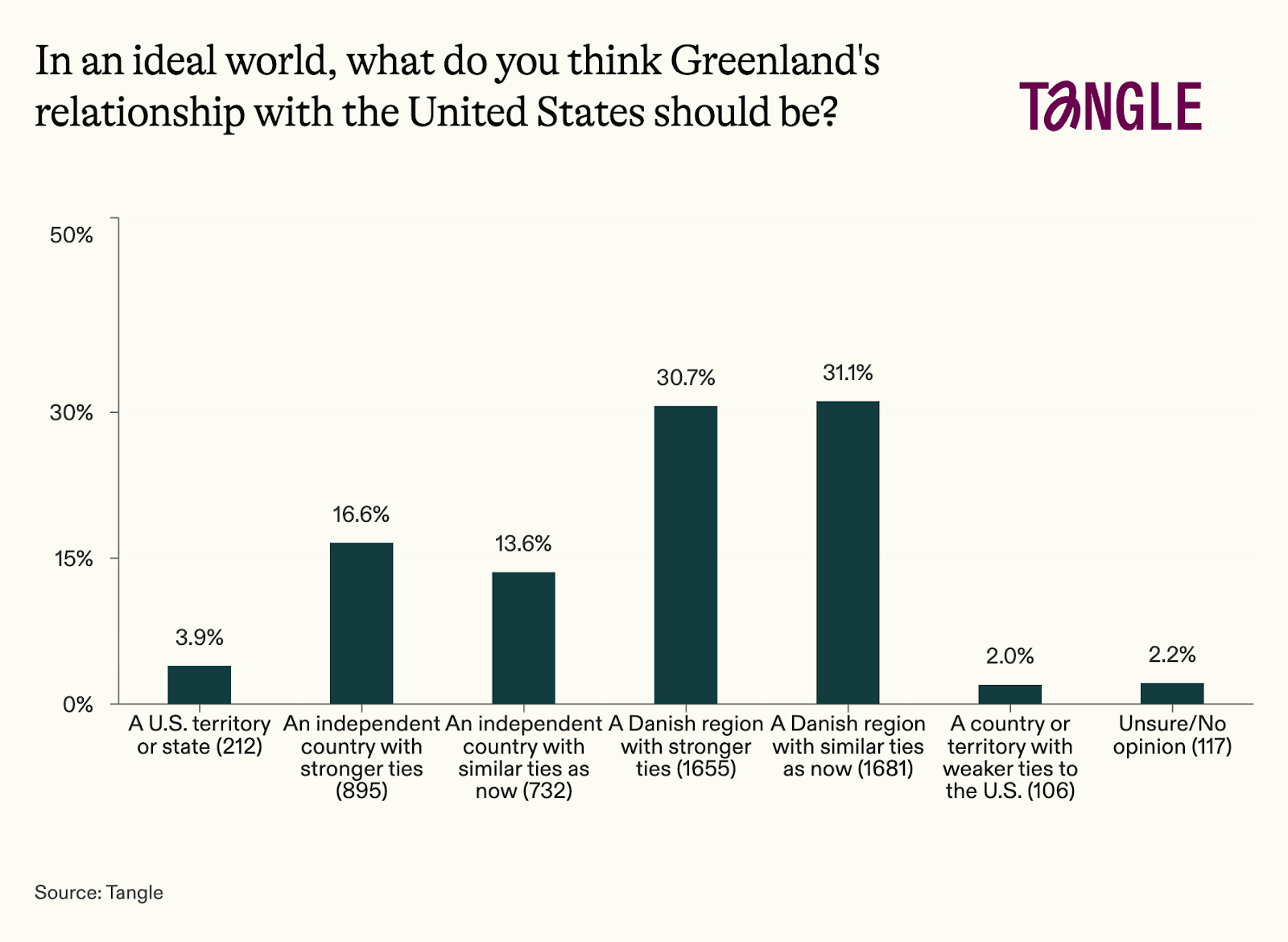
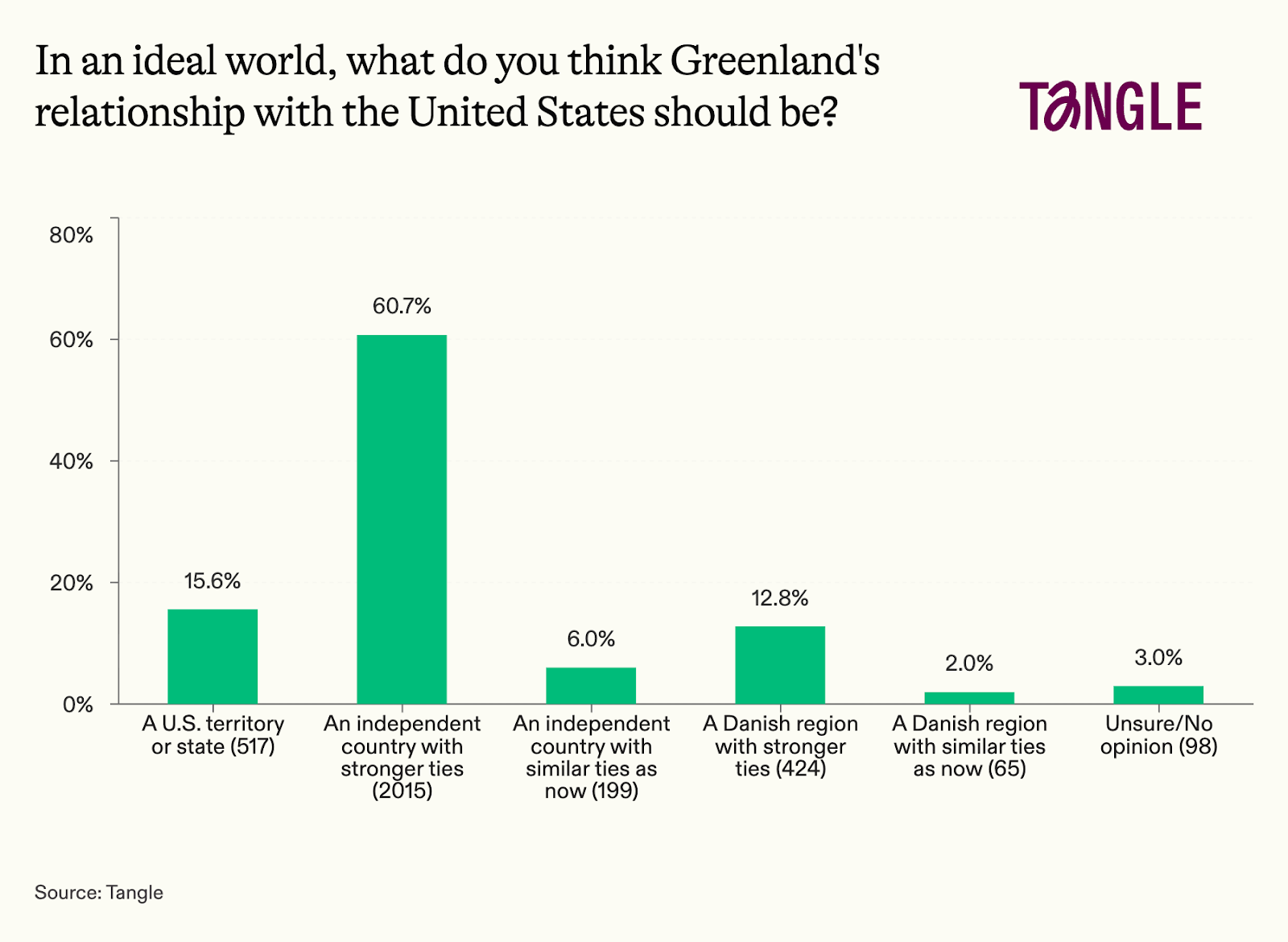
We asked the same question, with slightly different response options, on January 14, 2025. Those results, with 3,318 respondents, are shown below.
Have a nice day.
The American Cancer Society (ACS) projects that over two million people will be diagnosed with cancer in 2026, and the disease continues to be a leading cause of death in the U.S. But new ACS data released on January 13 showed two promising trends: Survival rates for more fatal cancers have improved dramatically over the past few decades, and, for the first time ever, 70% of people diagnosed with cancer live at least five years after their initial diagnosis. ACS’s chief scientific officer, Dr. William Dahut, identified available treatments, earlier screenings, and a drop in tobacco usage as contributors to the rising survival rates. “It’s really an exciting point. If we went back to the 1970s, less than half the people would be cancer-free or surviving at five years,” Dahut said. ABC News has the story.

Member comments